Why Dental X-Ray AI Accuracy Is Only as Good as the Sensor
· David Hanning
The latest generation of Direct Conversion sensor technology — and why “garbage in, garbage out” is the constraint nobody mentions in the AI pitch.
If you’ve talked to a chat bot this week, you’ve used AI. If you’ve called customer service, you’ve used AI. AI is in your phone, your inbox, your Google search, and — increasingly — your dental radiograph reader.
The pitch from the AI dental software vendors is consistent: better diagnostic accuracy, faster reads, fewer missed lesions, more confident treatment plans. Most of that pitch is technically true. It also misses the part of the equation that determines whether the AI you bought actually delivers what it promised.
Here’s the part that doesn’t make the brochure: AI is only as good as the image you feed it. And almost every intraoral sensor in the dental market right now is feeding it a modified image.
How Dental AI Actually Reads an X-Ray
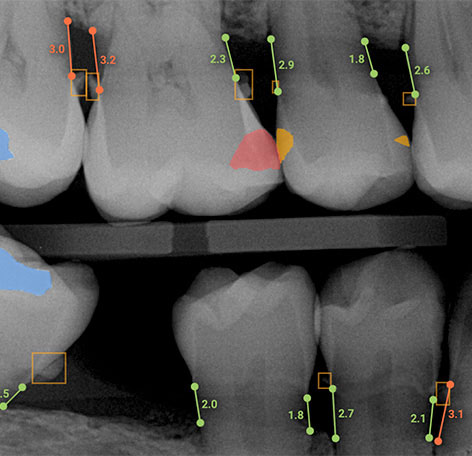
The basic mechanism is straightforward. The AI software receives a radiograph and identifies anatomical features — teeth, missing teeth, bone levels, apices, restorations. Then, based on training data labeled by practicing dentists, the AI marks areas of suspected pathology. The clinician can toggle the annotations on or off — useful for the chairside conversation with the patient, useful for confirming the AI’s call against your own read.
Figure 1. AI annotations on a dental radiograph identifying anatomy and flagging suspected pathology. Annotations can be toggled on or off for chairside patient education.
The training process for an AI engine is brute-force pattern recognition. A database of thousands of varied x-rays is assembled. Four or five practicing dentists go through each image and label the anatomy and pathology independently. They then come together and reconcile their individual reads into a “base truth” — the consensus interpretation that gets fed back into the model. Repeat across thousands of images. The AI learns to read x-rays the way the panel reads them.
When the AI works, it works well. It catches incipient caries a busy clinician might miss on a long day. It flags periapical changes too subtle to register on a quick screening read. It saves time and adds a second set of eyes that doesn’t get tired by Friday afternoon.
The “garbage in, garbage out” problem nobody is talking about
Here is the trade-off the vendors don’t lead with. The accuracy of AI diagnosis is highest when the AI is given predictable image information that has not been enhanced. That is not what most intraoral sensors deliver. The native image from a typical scintillator-based sensor (the architecture used by nearly every commercial sensor on the market today — fiber-optic plate or FOP sensors) is blurry — not because of poor manufacturing, but because of the physics of how the image is captured. Every commercial scintillator sensor solves that problem the same way: aggressive software enhancement applied to the image before you ever see it.
Sharpening filters. Edge detection. Contrast boosters. Different manufacturers call them different things and tune them at different levels, but the principle is identical. The pixel data gets modified to produce a visually appealing image at the monitor. The eye is fooled into thinking the image is sharper than it actually is.
For your eye, the enhancement is a feature. For the AI, the enhancement is a problem.
When the AI magnifies a region to inspect fine detail — say, the margin under an existing restoration — the enhancement filters distort what’s there. A sharpening artifact can read as an open margin when the actual pathology is recurrent decay. A contrast boost can erase the soft gradient that distinguishes sound dentin from incipient demineralization. The AI is doing exactly what it was trained to do; the input it’s working with is no longer faithful to what’s in the patient’s mouth.
What enhancement looks like when you zoom in past the point the eye is fooled
The same margin under an existing restoration, captured by different scintillator sensors and magnified to inspection level:
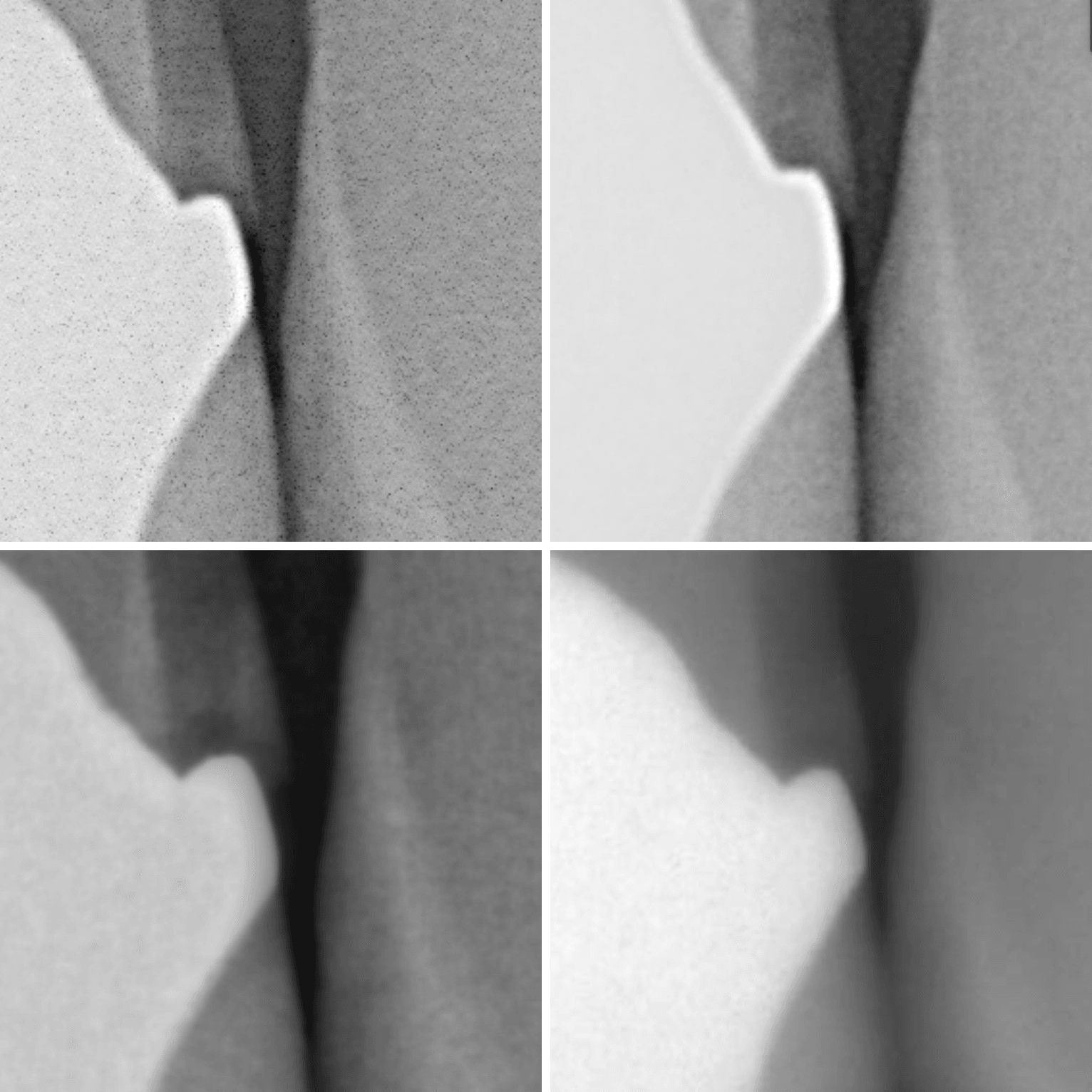
Figure 2. The same area of recurrent decay, captured by different scintillator-based sensors. Each manufacturer’s sharpening filter creates a different artifact pattern. AI trained across all of these is trying to hit a moving target.
Why image enhancement breaks AI accuracy at the source
The deeper problem is the training data itself.
Every AI dental engine on the market was trained on images that were also enhanced — thousands of them, from dozens of different sensor manufacturers, each with its own sharpening profile. The training panel of dentists labeled what they saw on enhanced images. The “base truth” the AI learned was a base truth filtered through enhancement.
So now we have AI trained on enhanced images, being fed enhanced images at the chair, with the enhancement varying by sensor brand, model year, and firmware version. The AI is doing pattern recognition across a moving target. It can’t always tell the difference between a real pathology and a sharpening artifact, because in its training data the two looked identical often enough to confuse the model. This is the “garbage in, garbage out” problem stated honestly. It’s also why a recent survey reported that 95% of dentists say they don’t trust AI to read their radiographs. The dentists are not wrong. The accuracy claims are real in the lab and unreliable at the chair, and clinicians can tell the difference even when they can’t articulate why.
 If you cannot see it, AI cannot either. AI needs IA “Image Accuracy”
If you cannot see it, AI cannot either. AI needs IA “Image Accuracy”
What direct conversion fixes — and why it matters chairside
Here’s the part of the story I’m closest to, because I helped build the solution.
Every commercial intraoral sensor for the last thirty years has used the same architecture: an X-ray hits a scintillator material, the scintillator converts the X-ray into visible light, the visible light spreads laterally as it travels, and a photodiode array beneath the scintillator captures the light. That lateral spread is what makes the native image blurry. The sharpening filters exist to compensate.
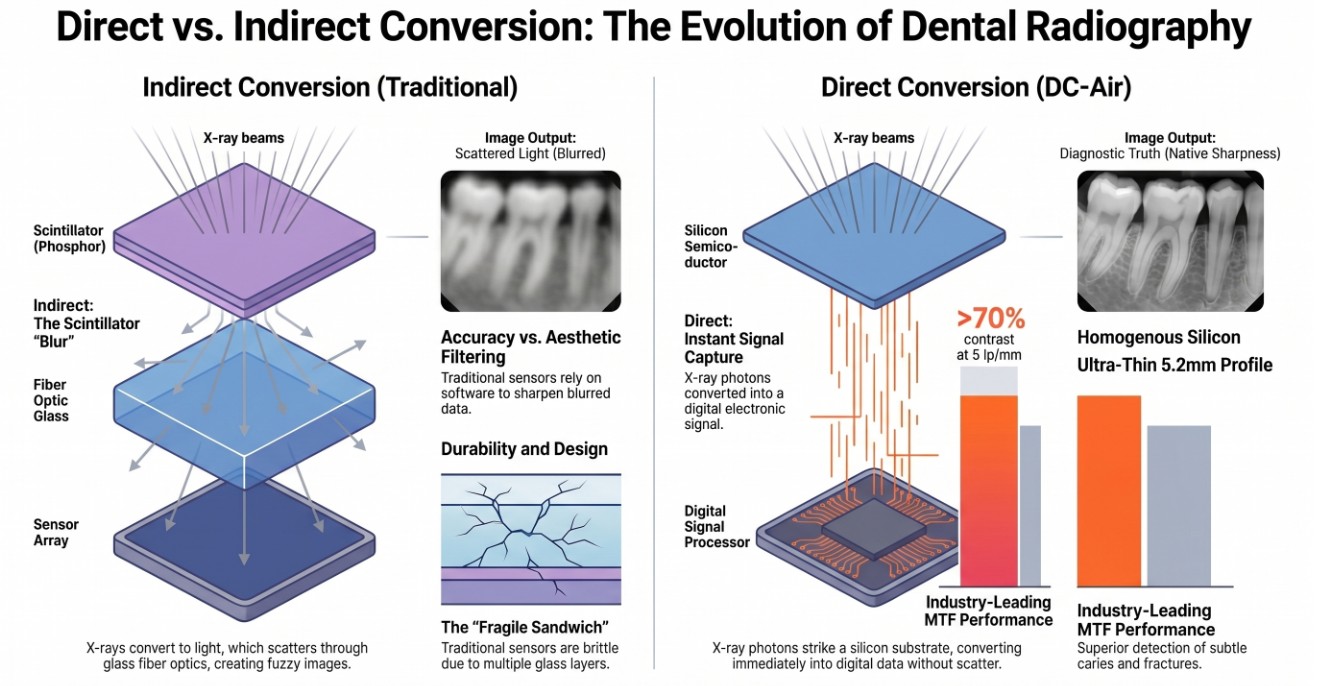 Figure 3. Comparison of indirect and direct conversion in dental radiography highlights the advantages of direct conversion. This method offers instant signal capture and higher image clarity without the blurring or fragility issues seen in traditional systems.
Figure 3. Comparison of indirect and direct conversion in dental radiography highlights the advantages of direct conversion. This method offers instant signal capture and higher image clarity without the blurring or fragility issues seen in traditional systems.
Direct Conversion skips the scintillator step entirely. The X-ray hits a single-crystal silicon CMOS detector and converts directly to electrical signal at the point of interaction. No visible light. No lateral spread. No need for downstream sharpening to compensate.
The result is a natively sharp image with 100% accurate pixel information — what the X-ray actually saw, captured in 26 μm pixels at 12-bit depth, no enhancement required.
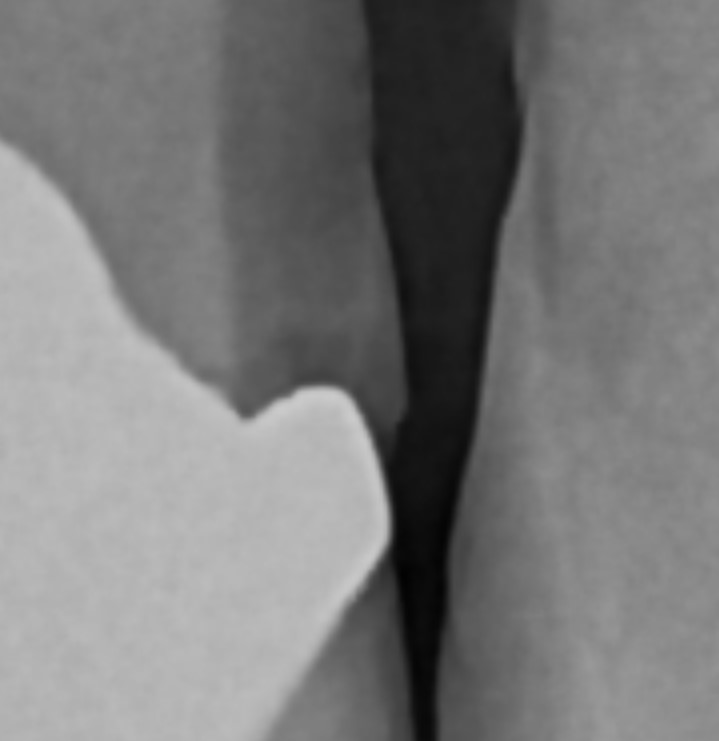
Figure 4. Native, unmodified detail from the DC-Air™ Direct Conversion sensor. Notice the organic shape of the decay and the continuous grayscale variation in the magnified view. The boundaries are where the actual pathology ends, not where a sharpening filter decided to draw a line.
Look at the magnified region in Figure 4. The shape of the decay is organic. The grayscale variation is continuous. The boundaries are where the actual pathology ends, not where a sharpening filter decided to draw a line. Compare that against the geometric shapes in Figure 2 — that is what enhancement looks like when you zoom in past the point the eye stops being fooled.
The DC-Air™ is the world’s first Direct Conversion intraoral sensor. We built it because the next generation of dental AI is going to need this — not as a nice-to-have, but as the only way the accuracy claims become true at the chair instead of just in the lab. In 2025 it won both the Dental Advisor Top Award and the Dental Product Shopper Best Product — two independent panels of practicing dentists evaluating it under separate testing protocols and reaching the same conclusion.
What’s next for AI in intraoral X-ray
AI in dental imaging is going to keep getting better. The training datasets will grow, the models will sharpen, the user interfaces will become harder to ignore. None of that changes the underlying constraint: the AI’s diagnostic ceiling is set by the quality of the image at the input.
 AI for Dental X-ray Needs IA “Image Accuracy” Like This Image Taken with the DC-Air™
AI for Dental X-ray Needs IA “Image Accuracy” Like This Image Taken with the DC-Air™
If the future of dental AI is going to live up to the marketing, the sensor side of the chain has to catch up. Direct Conversion CMOS is the architecture that lets that happen. Native pixel accuracy in, accurate AI diagnosis out. No filters in between, no artifacts to confuse the model, no “we’re not sure if that’s a margin or a sharpening line” pause at the chair.
The dentists who said they don’t trust AI today are right based on what’s been put in front of them. The same dentists will trust AI tomorrow when they see what it does with an image that hasn’t been modified before it reached the model.
The future of AI in intraoral X-ray is bright. It just needs the image to be honest first.
About the author. David Hanning is co-founder of FTG Imaging, the company that designed and manufactures the DC-Air™ Direct Conversion intraoral sensor, and CEO of Dental Technology Integrators (Dental TI). He has spent more than thirty-three years in dental imaging. The DC-Air won both the 2025 Dental Advisor Top Award and the 2025 Dental Product Shopper Best Product.
If you want to see how Direct Conversion changes what AI does with your radiographs — bring me your hardest case. I’ll join the demo. Talk to David about DC-Air →